Otitis Media With Effusion
WHAT IS OTITIS MEDIA WITH EFFUSION (OME)?
OME, otherwise known as ‘Glue Ear’, is the collection of fluid in the middle ear. It occurs commonly in children and up to 60% of children having at least one episode by age 6 has been quoted in studies. It frequently happens after an upper respiratory infection (flu) and in the majority of cases, it resolves by itself. The length of time for the resolution varies and may take up to 3 months. Studies have shown that 95% of the children would have complete resolution without any surgical intervention in 3 months.
WHAT CAUSES OME?
The problem is usually due to the malfunction of the eustachian tube. The eustachian tube connects the middle ear to the back of the nose which allows ventilation and proper function of the middle ear mechanism. In young children under the age of 10, the eustachian tube may be softer and more prone to blockage due to its immaturity. As a child grows, the eustachian tube stiffens and strengthens, reducing the frequency of fluid in the ear issues. Most children do not have middle ear issues after their first decade.
WHAT ARE THE SIGNS AND SYMPTOMS OF OME?
Older children often complain of earache and hearing loss. Younger ones may become fussy, sleep poorly, and often pull and tug at the ear. However, most of the time, the children are unaware of the hearing loss. The caregiver may notice that the child turns up the volume of the radio/TV or is not attentive during normal conversation. Teachers may also complain that the child is inattentive during lessons or is doing poorly in school.
HOW IS OME DIAGNOSED?
Fluid in the ear can be diagnosed in several ways. Very often, on clinical examination, the ear drums are found to be dull and sometimes bubbles of air may be seen behind them (Figure 1). Audiogram typically shows a mild to moderate conductive hearing loss. Tympanogram may also show a type ‘B’ (Fig. 2) tracing as opposed to a normal type ‘A’ (Fig. 3).

Figure 1. Middle ear effusion seen behind the ear drum. Presence of yellow fluid with air bubbles.
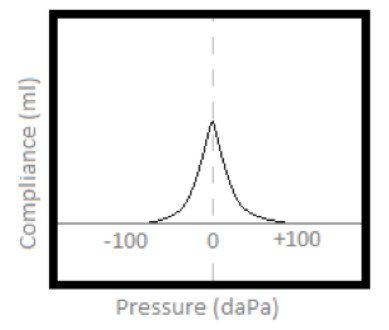
Figure 2. Type A tympanogram indicating an air-filled middle ear
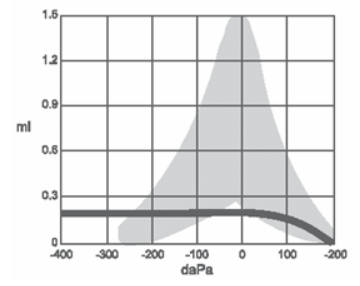
Figure 3. Type B tympanogram indicating a fluid-filled middle ear or other middle ear pathologies resulting in reduced compliance of ear drum
WHEN SHOULD IT BE TREATED?
When symptoms of hearing loss persist, particularly at a time when a child is learning to speak, medical evaluation and treatment are recommended. Hearing loss is the single most important cause of a child having delayed speech.
TREATMENT OPTIONS
To improve eustachian tube function, a variety of medications may be used. Antibiotics, decongestants and nasal sprays (if nasal allergy co-exists) are the more common ones. If this fails, otitis media with effusion treatment may involve surgical options. For children, the operations performed are Myringotomy & Tube insertion (M&T) with or without adenoidectomy.
SURGERY
M & T is done under general anaesthesia as a day surgery. This simple procedure generally takes about 15 minutes and involves making a cut on the ear drum and placing a tiny ventilation tube through it. This then allows ventilation of the middle ear and prevents the accumulation of fluid in the middle ear. Possible admission to the hospital is required only when adenoidectomy is performed at the same setting. Your child may be required to fast overnight (no food or drink after 12 midnight) before the operation. For a younger child, a shorter period of fasting might be sufficient, depending on the anaesthetist’s assessment.
PREPARATION FOR SURGERY
The doctor should be informed if your child has fever and cough just before the surgery. The surgery might be postponed if the child is found to be unfit for surgery. If the child has any history/family history of bleeding disorder or any previous problems with anaesthesia, it should be brought to the doctor’s attention.
SOON AFTER SURGERY
The child might still be sleepy and have vomiting from the effects of general anaesthesia. After a few hours, he/she will be allowed to drink water. Eating will resume depending on the child’s recovery. An immediate improvement in hearing should follow after surgery. There is no dietary restriction and normal diet and oral hygiene should resume.
AFTER DISCHARGE
We would like to review your child 2-4 weeks after the surgery. Do keep your appointment with the doctor as the follow-up care is important to ascertain extrusion of the tube and if there is recurrence of middle ear fluid.
The ventilation tubes placed through the eardrum will be automatically expelled in 6-18 months. This might need removal by the doctor from the ear canal in the clinic during a follow-up visit.
If the child experiences purulent ear discharge or pain after the operation, please do give our clinic a call for an early consultation. This may occur when the child has an upper respiratory tract infection sometime after surgery and with a patent and functioning grommet tube.
PRECAUTIONS
Keep the ears dry as water in the middle ear increases the chance of infection. Do not allow shower spray to be directed into the ears. Older children will still be able to swim but this should be done while wearing good ear plugs. Placing of the head under water is to be avoided. Diving or swimming should be avoided in children below age 6. In the event of an ear infection, where there is pus discharging from the ears, medical opinion should be sought.
Usually post-operative reviews in 1 month are given. Please keep your appointment as follow-up care is important to ascertain extrusion of the tube and if there is a recurrence of middle ear fluid.
Related Doctor

Dr Annette Ang Hui Chi
Senior Consultant Ear, Nose and Throat MBBS (Singapore), MRCS (Edinburgh), MMed (ORL), FAMS (ENT)Related Articles

Hepatitis Can Be Silent: Would You Know If You Had It?
July 28, 2026
Loneliness in Older Adults: Why It’s a Mental Health Issue, Not Just Social
July 21, 2026